
You're tracking calories. You're following a meal plan. You're eating "1,500 calories" because that's what the calculator said. But the scale isn't moving—or worse, you're gaining weight. The problem isn't your discipline. It's that you're working with a number that was never actually yours.
Most people diet using estimated calorie targets from online calculators. Those calculators give population averages, not individual measurements. If your actual resting metabolic rate (RMR) is 1,300 and you're eating 1,500 "for weight loss," you're in a surplus. If your RMR is 1,900 and you're eating 1,500, you're undereating so severely that your metabolism is adapting downward.
Without knowing your actual RMR, every calorie decision is a guess.
What RMR Actually Is (And Why It's Not What You Think)
Resting metabolic rate is the number of calories your body burns at rest—no activity, just existing. Breathing, circulating blood, regulating temperature, repairing cells, maintaining organ function. This isn't the same as basal metabolic rate (BMR), which is measured in clinical sleep conditions. RMR is slightly higher and more practical to measure because it reflects normal resting state, not deep sleep.
Here's what matters: RMR accounts for 60-75% of your total daily calorie burn. It's the foundation of all calorie calculations. Your total daily energy expenditure (TDEE) is RMR plus activity. If your RMR estimate is wrong, your entire calorie strategy is wrong.
And RMR is highly individual. Two people—same age, same height, same weight—can have RMRs that differ by 300-500 calories. Research shows that standard calorie prescriptions based on weight alone can be significantly off, with women and certain demographics consistently assigned higher calorie goals than their actual RMR would indicate.
Population averages don't apply to individuals. Using an equation based on your demographics might land you in the ballpark—or it might miss by hundreds of calories per day.
Why Online Calculators Fail
Calorie calculators use equations like Mifflin-St Jeor or Harris-Benedict. These were developed from population data and estimate RMR based on age, weight, height, and sex. They're useful for research. They're not precise enough for individuals.
What they can't account for:
- Muscle mass: More muscle = higher RMR. Two people weighing 150 pounds can have vastly different RMRs if one carries 120 pounds of lean mass and the other carries 100.
- Metabolic adaptation from past dieting: Chronic dieters have suppressed RMR. If you've lost and regained weight repeatedly, your RMR is likely lower than predicted.
- Thyroid function: Even subclinical hypothyroidism lowers RMR. Calculators assume normal thyroid output.
- Genetic variance: Some people naturally burn more or less at rest. Equations can't capture this.
Studies show that measured RMR can differ from predicted RMR by 20-30% in either direction. That's not a rounding error. That's the difference between weight loss and weight gain on the same calorie intake.
You follow the calculator. You eat the "right" amount. You don't lose weight. You assume you're doing it wrong. You cut calories more. You worsen metabolic adaptation. The cycle continues.
The calculator isn't right or wrong—it's just an estimate. And estimates don't work when precision matters.
What Happens When You Eat Below Your RMR
Here's what most people don't understand: your body doesn't know you're "on a diet." It just knows you're not eating enough. And when you consistently eat below your resting metabolic rate—the baseline calories your body needs just to keep you alive—it doesn't think "oh, she's trying to lose weight." It thinks "we're starving. We need to survive."
When you eat significantly below your RMR for weeks or months, your body activates survival mode. It does two things:
First, It Slows Down
Your metabolism decreases to match the lower calorie intake. This is called metabolic adaptation (or adaptive thermogenesis, if you want the scientific term). Research on adaptive thermogenesis shows that weight loss triggers physiological changes designed to conserve energy and accelerate fat storage during weight regain.
Your thyroid function drops—specifically, your body produces less active thyroid hormone (T3), which regulates metabolic rate. Your leptin levels (the hormone that signals "we have enough energy") plummet, which further suppresses calorie burn and increases hunger. Studies show that very low calorie dieting causes resting metabolic rate to decrease, making it progressively harder to lose weight and easier to regain it.
Second, It Hoards
Your body becomes hyper-efficient at storing any calories it does get. When you eat slightly more—even if you're still technically in a deficit according to your old RMR—your body prioritizes fat storage over fat burning. This is why people who chronically undereat often gain weight when they return to "normal" eating. Their RMR has dropped so low that what used to be maintenance calories is now a surplus.
Research confirms that people losing larger amounts of weight experience RMR declines greater than what can be accounted for by loss of lean mass alone—meaning metabolic adaptation is real, measurable, and significant.
Real-World Example
Let's say your actual RMR is 1,400 calories. You don't know this, so you follow an online calculator that says eat 1,200 for weight loss. You do this for three months.
Initially, you lose weight. But then you plateau. You're eating 1,200 calories—barely anything—and the scale won't budge.
What happened? Your body adapted. Studies show that RMR can decrease by approximately 100 calories per day following moderate weight loss, with 40% of this reduction attributed to metabolic adaptation rather than tissue loss. Your RMR dropped from 1,400 to maybe 1,250 or even 1,200. You're now maintaining your weight on 1,200 calories, not losing. Your metabolism slowed to match your intake.
When you inevitably can't sustain 1,200 calories forever and go back to eating 1,500—which should still be a modest intake—you gain weight rapidly. Because your RMR is now 1,200, eating 1,500 puts you in a 300-calorie surplus.
This is why chronic dieters often say "I gain weight eating 1,400 calories, but I used to lose weight on 1,800." It's not that they're lying or doing it wrong. Their RMR changed. And they never measured it.
The Survival Mechanism
The body's survival mechanism doesn't care about your weight loss goals. When you eat below your RMR consistently, you trigger adaptive thermogenesis—a fancy term for "your metabolism slows down to match what you're eating." The lower you go, the more your body fights back by:
- Decreasing thyroid output (less T3 = slower metabolism)
- Lowering leptin (hunger increases, calorie burn decreases)
- Increasing cortisol (stress hormone that promotes fat storage, especially around the midsection)
- Reducing non-exercise activity thermogenesis, or NEAT (you unconsciously move less—fidget less, take fewer steps, expend less energy in daily tasks)
Your body becomes a calorie-hoarding machine. And the worst part? You can't feel this happening. You don't wake up and think "oh, my RMR just dropped 200 calories." You just notice you're not losing weight anymore despite eating very little.
This isn't "metabolic damage" or a "broken metabolism." It's your body doing exactly what it's designed to do: adapt to perceived starvation by conserving energy and storing fat for survival.
But you can't reverse what you can't measure. If you don't know your current RMR, you don't know if you're eating too little (triggering adaptation), eating at maintenance (no change), or eating in an actual deficit (productive weight loss).
What Happens When You Eat Above Your RMR (But Think You're in a Deficit)
Now let's flip the scenario. What if your RMR is actually lower than the calculator estimated—and you're eating more than you think you need?
The Math Problem
Say your actual RMR is 1,300 calories. But the online calculator—using your age, weight, and height—estimates it at 1,600. You're told to eat 1,500 calories for "gradual weight loss" (a 100-calorie deficit from the estimate).
But if your real RMR is 1,300, you're not in a deficit. You're in a 200-calorie surplus. Every day. Over a month, that's 6,000 extra calories—nearly two pounds of fat gain.
You're doing everything "right" according to the plan. You're tracking. You're hitting your target. But you're gaining weight. And you have no idea why.
Why This Happens
- Metabolic adaptation from past dieting: If you've dieted repeatedly, your RMR might be suppressed. Calculators don't account for this.
- Lower muscle mass: Muscle burns more calories at rest than fat. If you've lost muscle (from crash dieting, aging, or inactivity), your RMR is lower than average for your weight.
- Thyroid issues: Even subclinical hypothyroidism can lower RMR by 10-20%. Calculators assume normal thyroid function.
- Genetic variance: Some people just naturally have slower metabolisms. Population averages don't capture outliers.
The Frustration Cycle
You eat what the plan says. You gain weight. You assume you're "eating too much" or "miscounting calories." So you cut more. Now you're eating 1,300—right at your RMR. You stop gaining, but you don't lose either. You're stuck.
Eventually, you cut to 1,200. Now you're below your RMR. Metabolic adaptation kicks in. Your RMR drops further. The cycle continues.
You don't have a "slow metabolism." You have an unmeasured one. And without measurement, you're flying blind.
Why RMR Changes Over Time (And Why You Need to Remeasure)
RMR isn't static. It changes with age, body composition changes, weight loss, chronic dieting, and hormonal shifts. Research shows that energy expenditure is highly affected by weight changes, playing a significant role in weight regain and metabolic resistance.
What changes RMR:
- Age: RMR declines approximately 2-3% per decade after age 30, primarily due to loss of lean muscle mass.
- Muscle loss: Less muscle = lower RMR. Muscle is metabolically active tissue. Fat is not.
- Weight loss: A smaller body requires fewer calories. But the RMR drop is often greater than expected based on weight loss alone due to metabolic adaptation.
- Chronic dieting: Repeated cycles of weight loss and regain suppress RMR over time. Studies of participants from "The Biggest Loser" showed persistent metabolic adaptation 6 years after competition, with RMR remaining significantly lower than predicted despite partial weight regain.
- Hormonal changes: Menopause, low testosterone, hypothyroidism all lower RMR.
The Key Insight
The RMR you had five years ago isn't the RMR you have now. What worked then won't work now.
Example: You lost 20 pounds eating 1,600 calories five years ago. Your RMR was 1,800 then. Now it's 1,500. Eating 1,600 is now maintenance, not a deficit.
You're not failing at the same diet. You're using outdated data.
How RMR Testing Actually Works
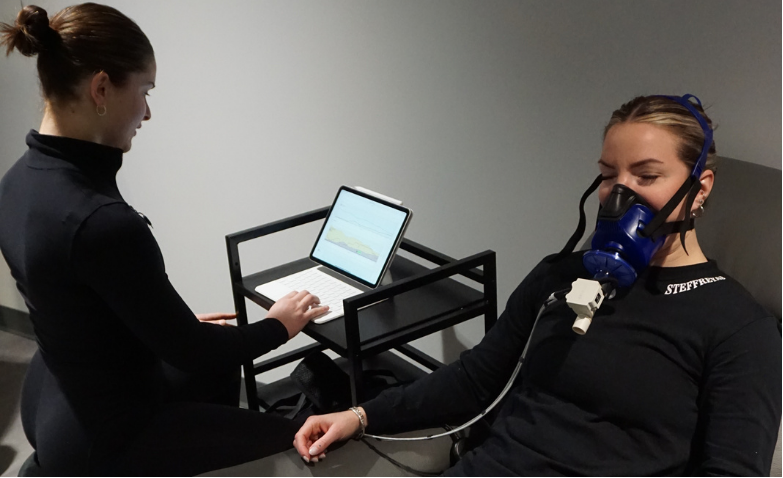
RMR is measured via indirect calorimetry—a breath-by-breath analysis of oxygen consumption and carbon dioxide production. PNOĒ metabolic testing uses this method to reveal your exact calorie burn at rest.
The test takes 8-10 minutes. You breathe normally into a mask while at rest. The system measures how much oxygen you consume and how much CO2 you produce. From this, it calculates your precise RMR—not an estimate based on population averages, but YOUR number.
What You Learn
- Actual RMR: The exact number of calories you burn at rest
- Comparison to predicted values: Whether your RMR is high, low, or average for your demographics
- Evidence of metabolic adaptation: If your RMR is significantly lower than predicted, you've likely experienced adaptive thermogenesis from past dieting
- Substrate utilization: How much fat vs. carbohydrate you burn at rest (indicates metabolic flexibility)
Once you know your RMR, you can set accurate calorie targets. Deficit = RMR + activity - X calories. No guessing.
What to Do Once You Know Your RMR
If RMR Is Lower Than Expected (Metabolic Adaptation)
Don't cut calories further. You're already undereating, which is why your RMR suppressed.
Consider reverse dieting: gradually increase calorie intake to restore RMR. This takes patience—weeks to months—but allows your metabolism to recover before attempting another deficit.
Address underlying causes: Get thyroid tested (comprehensive blood panels measure TSH, free T3, free T4). Evaluate chronic stress (high cortisol suppresses metabolism). Ensure you're not overtraining.
Retest after intervention to confirm metabolic recovery. Don't assume your RMR has normalized—measure it.
If RMR Is Higher Than Expected
Good news: you can eat more and still lose weight. Adjust calorie targets upward. Avoid unnecessary restriction.
Use an accurate deficit instead of generic "1,200 calories." If your RMR is 1,900, eating 1,600-1,700 creates a sustainable deficit without triggering adaptive thermogenesis.
If RMR Is Normal But Weight Loss Stalled
The problem likely isn't RMR. Check:
- Activity tracking accuracy: Are you overestimating calorie burn from exercise?
- Food logging accuracy: Are portions precise, or are you underestimating intake?
- Hormonal factors: Combine RMR testing with blood work to assess thyroid, cortisol, and sex hormones.
Testing removes guesswork. You either have data showing where the problem is, or you can rule out metabolic issues and look elsewhere.
Stop Guessing. Start Measuring.
PNOĒ metabolic testing measures your resting metabolic rate, VO2 max, and substrate utilization in 8 minutes. Know exactly how many calories your body burns—and whether metabolic adaptation is sabotaging your weight loss.
Book Your Metabolic Test